The Hot Potato of Healthcare

Amanda DeMarzo
Jul 18, 2020
7 minutes read

Prior Authorizations are complicated for everyone involved. As a patient who doesn’t know much about the administrative requirements of a doctor’s office, it must feel like a game of hot potato. It constantly goes around and no one seems to want it. Patients are making calls to the physician, pharmacy, and insurance company with no idea what is going on. Someone instructed them to say certain words and see what happens.
Some find themselves asking, “Is everyone else calling around? Is everyone else stuck in a never-ending phone call trying to find the right person to speak to?”
Let’s start at the beginning:
What is a Prior Authorization
A prior authorization is a complex process that is put in place to reduce costs for an insurance company and the patient. Sometimes it is used to “double-check” a provider’s health decision through medical necessity. Medical necessity is the buzz word for checking if it is the appropriate next step in care or if there is something else that is more or equally effective.
Panels of experts in specific disease states develop guidelines to determine what is the appropriate and effective algorithm of care. It is determined by clinical trial data as well as real-world data and experiences. The clinical guidelines change as clinical information becomes available.
- For example: Diabetes algorithm changed when studies showed that some medications have long-term cardiovascular benefit. These drugs are now preferred because it reduces risk of a cardiovascular event, such as high blood pressure or stroke.
Insurance companies then use these guidelines and cost evaluation to determine what medications they would prefer to pay for. Costs can be determined by market price or discounts from manufacturers based on the volume of customers on that medication. Therefore, some insurance companies may prefer brand drugs or more expensive drugs over generic alternatives.
The need for medical necessity can also be dictated by the insurance company. Cost-saving measures and processes can be implemented in this requirement. For example, step therapy and fail-first therapies can be required before moving on to the more expensive treatment option.
Step therapy, also known as fail-first therapy, is the process in which patients must try certain treatments before moving on to something that is likely more expensive. A patient may have to use three or more other therapies before something with better efficacy due to the cost. This can delay care and be detrimental to their disease management in many cases.
How does a Prior Authorization get processed?
From many patients’ perspectives, the prior authorization starts at the pharmacy. Little do they know; a similar process is used for authorization of services and procedures.
Their doctor gave them a prescription that they want to fill to feel better. The patient took that prescription to the pharmacy and the pharmacy said no. Someone at the pharmacy then says the insurance is rejecting it because the doctor needs to submit more information to get approval.
What type of information is needed? Why didn’t the doctor mention this possibility? Is this normal? Shouldn’t the doctor know if more information is needed? There are a lot of questions going through the patient’s mind.
The answer to all of these questions comes down to one thing: doctors do not know which medications need prior authorizations when you leave the office. There are many insurance companies and they all have different requirements for coverage and payment. The doctor usually does not know until the patient finds out at the pharmacy.
The prior authorization is a complex process with many stakeholders. Again, this can feel like a game of hot potato. Everyone touches it but no one wants to hold on to it.
A simplified version of the prior authorization process looks like this:
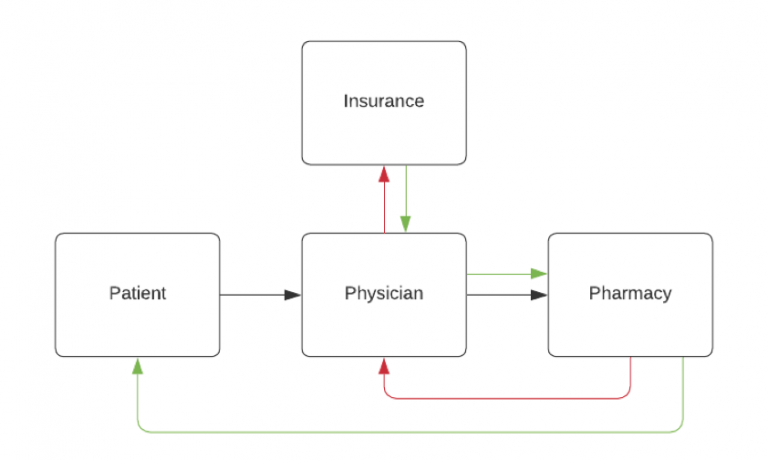
The black arrows represent the patient going to the physician then the pharmacy. The red arrows are the rejection and requirement of a prior authorization. The green arrows are the process of notifying everyone of the approval.
Except it isn’t this simple. Physician’s offices must track every prior authorization. Insurance companies do not actively notify providers or pharmacies of an approval. Physicians and staff need to access the insurance portal to see the status of the claim. If it receives approval, they then have to take another step to call the patient’s pharmacy to inform them it has approval. In this workflow, it is easy to skip the step of following up.
What may really be happening, may look more like this:
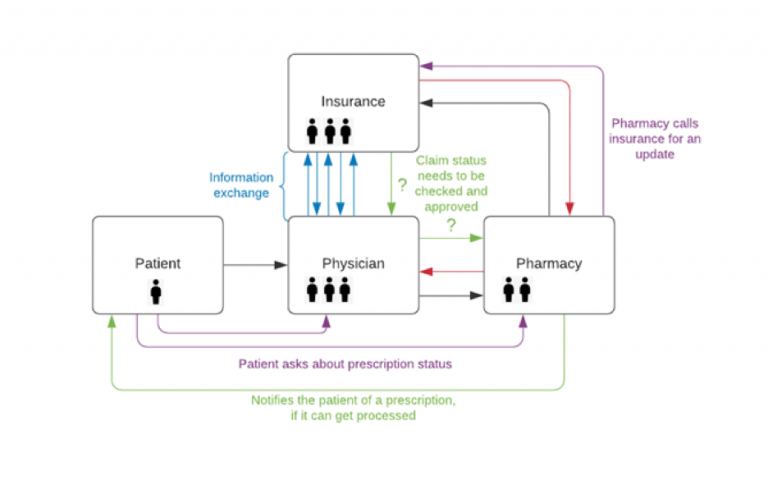
This whole process can take days or weeks to complete. One misstep, mistake, or missing follow-up and the whole process can be disrupted.
How do we improve?
In a 2019 AMA Survey of physicians, it was discovered that each physician is spending approximately 14.4 hours per week on prior authorizations. That means for every 2.7 physicians, there should be one staff member entirely dedicated to prior authorizations. Yet, only 30% of physicians report having dedicated support staff to help with this administrative burden.
The long-term goal is to increase the number of support staff available to help with prior authorization. Additionally, improving competency in this area through certification will also reduce the time spent on processing prior authorizations.
We want to stop playing hot potato. Stop passing prior authorizations around until they eventually receive approval. We need dedicated Prior Authorization Certified Specialists who are capable and ready to hold on to that hot potato until the claim gets approval. Patients need advocates who will fight for their care.